June was a month of advocacy, collaboration, and progress across the FH Europe Foundation network, with important developments in EU policy, rare disease advocacy, research, and patient engagement. As summer begins, our community continues to drive forward early detection, prevention, and equitable care for inherited lipid disorders.
Catch up on the key highlights from the June 2026 edition of Heart Beat:
FH Europe Foundation News:
- Early Screening for Inherited Lipid Disorders: Continued advocacy for inclusion in future EU Cardiovascular Health Checks.
- HTAi Annual Meeting 2026: Contributing the patient perspective to discussions on health technology assessment and prevention.
- HoFH Webinar Trilogy: Exploring diagnosis, treatment advances, and lived experience.
- Lp(a) Update 2026: Advancing collaboration on testing, prevention, and implementation.
- Rare Disease Advocacy: FHEF joins Rare Diseases International and the European Regional Task Force on Rare Diseases.
- FHEF Annual Network Meeting in Dublin: Registration details to be announced soon.
Ambassador Programme News:
- Ambassadors at Key Events: Bringing the patient voice to international conferences, meetings, and webinars.
Research & Community Engagement:
- PERFECTO at JACARDI Learning Session: Strengthening collaboration on health literacy, prevention, and patient empowerment.
- PERFECTO Project Legacy: Advancing paediatric FH screening across Europe.
- FH-EARLY at the LSEDL Annual Congress: Raising awareness of early FH identification and management.
Network News:
- Spain: SAFEHEART study highlights the long-term benefits of early FH treatment.
- Latvia: ParSirdi.lv supports innovation in FH diagnosis, awareness, and patient engagement.
- Spain: Corazón Sin Fronteras webinar explores women and cholesterol care.
- Singapore: FH Connect 2026 brings patients, families, and healthcare professionals together.
- Czech Republic: ČAKO promotes patient education and community-based prevention.
- France: Anhet.f webinar focuses on FH and Lp(a) diagnosis and management.
Partner News:
- EURORDIS: New evidence highlights the mental health impact of living with a rare disease.
- EURORDIS: Calling for stronger and more coordinated newborn screening programmes across Europe.
- Global Heart Hub: New insights into women’s experiences of cardiovascular care.
- BBMRI-ERIC: Supporting implementation of the European Health Data Space. Knowledge Hub
Knowledge Hub:
- EAS Paediatric FH Symposium Recordings: Expert perspectives on screening, diagnosis, and treatment.
- EUPATI Patient Expert Training Programme: Building patient advocacy and research expertise.
- Global Heart Hub Webinar: Exploring access to cardiac rehabilitation and long-term support.
- EUCAPA HTA Training: Strengthening patient involvement in health technology assessment.
- EMA Approval of Plozasiran: Expanding treatment options for people living with FCS.
Events:
- 28-31 August: ESC Congress 2026, European Society of Cardiology (ESC), Munich, Germany
- 15 September: Apheresis Awareness Day
- 24 September: FH Awareness Day
- 27-28 October: World Orphan Drug Congress, Amsterdam, The Netherlands
- 29 September: World Heart Day, World Heart Federation
- 6 November: FCS Awareness Day
- 6-8 November: FHEF Annual Network Meeting, Dublin, Ireland
At FH Europe Foundation, we believe that meaningful change begins by listening—truly listening—to the communities we represent. That is why we are proud to be part of an important new initiative led by
EURORDIS, in collaboration with
Rare Diseases International (RDI): the
establishment of a European Regional Task Force on Rare Diseases.
This is more than another working group. It is a significant step towards ensuring that the voices of people living with rare conditions, including homozygous familial hypercholesterolaemia (HoFH) and familial chylomicronaemia syndrome (FCS), are embedded in the policies that shape their care, treatment, and future. The Task Force has a clear and ambitious purpose: to contribute to the development of a European Blueprint for Rare Diseases. This Blueprint will serve as a multi-stakeholder framework designed to guide future action at both European and global levels. Its outcomes are expected to inform:
- The development of a future EU Action Plan on Rare Diseases, and,
- Regional recommendations from the WHO European Region, feeding into a Global Action Plan on Rare Diseases.
This positioning is critical. For years, the rare disease community has called for stronger, more coordinated policy action. While national plans have made progress, there remains fragmentation across countries, inconsistencies in care, and unequal access to diagnosis and treatment. The Blueprint—and the Task Force behind it—offers a chance to move from patchwork progress to aligned strategy. Inherited lipid conditions such as HoFH and FCS are often under-recognised in the rare disease space; it is still invisible and does not fit in the typical box. Initiatives like this ensure that:
By participating in this Task Force, FH Europe Foundation is helping to ensure that the realities of our community—early screening needs, family-based care, lifelong management—are reflected in wider rare disease discussions. However, participation alone is not enough. A critical question remains: Will this Task Force deliver meaningful influence, or risk becoming another consultative exercise? There is growing recognition across European health policy that patient involvement must go beyond “a seat at the table”. True engagement means:
- Patients are involved early, not after decisions are drafted
- Their contributions shape outcomes, not just discussions
- There is transparency on how input is used
The strength of this initiative will depend on how well it translates lived experience into actionable policy recommendations—and whether institutions are ready to act on them. The creation of a European Blueprint is a major opportunity, but it also comes with challenges that must be acknowledged:
Opportunities
- Alignment across Europe: A shared framework can reduce disparities between countries
- Stronger advocacy voice: A unified rare disease community carries more weight at EU and global levels
- Policy momentum: With WHO engagement, this work connects regional priorities to global action
Challenges
- Implementation gap: Policies are only as effective as their execution at national level
- Diverse needs: Rare diseases are heterogeneous, and balancing priorities across conditions is complex
- Sustained commitment: Political and financial support must extend beyond initial strategy development
For FH Europe Foundation, this means continuing not only to contribute to the discussion, but to champion the needs of our community—helping ensure that commitments made at European level translate into tangible improvements in people's lives.
Together with EURORDIS, RDI, and partners across the rare disease community, we remain dedicated to driving meaningful change. Central to this effort is ensuring that the voices of people living with HoFH, FCS, and other inherited lipid disorders, as well as their families, are not only heard but reflected in concrete actions and policies.
By bringing forward lived experiences, sharing evidence and insights from our key initiatives and EU-funded projects, and advocating for practical, measurable solutions, we aim to advance earlier detection, more effective prevention, and greater equity in care across Europe.
The establishment of the European Regional Task Force marks an important milestone—but it is only the beginning. The real measure of success will be whether this work leads to:
- Earlier diagnosis across Europe
- Better access to treatment
- More coordinated care pathways
- Stronger recognition of rare and genetic conditions in health policy
We will continue to engage actively in this process and keep our community informed as the Blueprint develops.
Together, we can ensure that European and global policies reflect the realities—and the needs—of those living with rare conditions.
May was a month of strong global engagement and policy momentum across our community, with key milestones at the World Heart Summit, World Health Assembly, and EAS Congress reinforcing the importance of early detection and prevention.
Looking ahead, growing EU policy discussions and continued collaboration across research, advocacy, and patient engagement signal an important period for advancing recognition of inherited lipid disorders and strengthening cardiovascular health systems.
Catch up on the key highlights from the May 2026 edition of Heart Beat:
FH Europe Foundation News:
- EU Call for Evidence on Cardiovascular Health Checks: FHEF submission and strong community mobilisation
- World Heart Summit: Bringing the patient voice to global cardiovascular discussions
- World Health Assembly (WHA79): Advancing prevention and early detection on the global stage
- EAS Paediatric FH Symposium: Focus on early detection and management in children
- EAS 2026 Congress: Strengthening science, policy, and patient partnerships
- Lp(a) International Task Force: Moving from awareness to implementation
Ambassador Programme News:
- Elsie Evans at EU Safe Hearts dialogue: Advocating for equity and patient-centred care
- Lena-Rosa Hanauer at Europe Biobank Week: Young patient voice in research discussions
- Patsy Petrie shares her FH journey on the Pioneering Patient Podcast
Research & Community Engagement:
- PERFECTO Capacity Building Workshop in Cyprus: Strengthening knowledge on FH screening and prevention
- PerMed FH Consortium meeting: Advancing precision medicine and genetic research
- FH-EARLY survey: Capturing patient experiences to improve care and support
Network News:
- China: FH China launches national survey on economic burden of HoFH treatment
- Italy: AISC announces cardiovascular prevention day in Rome
- Sweden: FH Sweden marks 10 years of progress in national FH care
- NEW: FH Iraq joins the FHEF Network
Partner News:
- EURORDFIS:Upcoming mental health activities
- Health Technology Assessment International: Lp(a) ITF joining the HTAi Annual Meeting in Istanbul
News from around the World:
- Croatia: “Run for Health” promotes prevention and healthy lifestyles among families
- UK: Genetic Alliance UK’s Future for Rare campaign calls for improved care for rare conditions
Knowledge Hub:
- EAS consensus statements: Advancing lifelong cardiovascular prevention and lipid care
- EU webinar: Youth engagement in cardiovascular prevention – registration open
- REMEDi4ALL Bootcamp: Training opportunity for patient representatives
Events:
- 2–4 June: PEOF 2026 Global Gathering
- 3–4 June: European Conference on Rare Diseases (ECRD 2026)
- 5 June: World Environment Day
- 8–10 June: HTAi 2026 Annual Meeting
- 28–31 August: ESC Congress 2026
We are pleased to announce the publication of two major European Atherosclerosis Society (EAS) consensus statements:
- Familial hypercholesterolaemia in children and adolescents
- Lipid clinics worldwide: harmonisation and guidance on how to optimally organize and fund
Both statements were published simultaneously on 25 May 2026 and presented during a joint session at the EAS Annual Congress 2026 in Athens, Greece.
These landmark publications represent important advances in early detection, prevention, and lifelong management of inherited lipid disorders and cardiovascular disease.
1.Advancing early detection and care of familial hypercholesterolaemia in children and adolescents: a consensus statement from the European Atherosclerosis Society
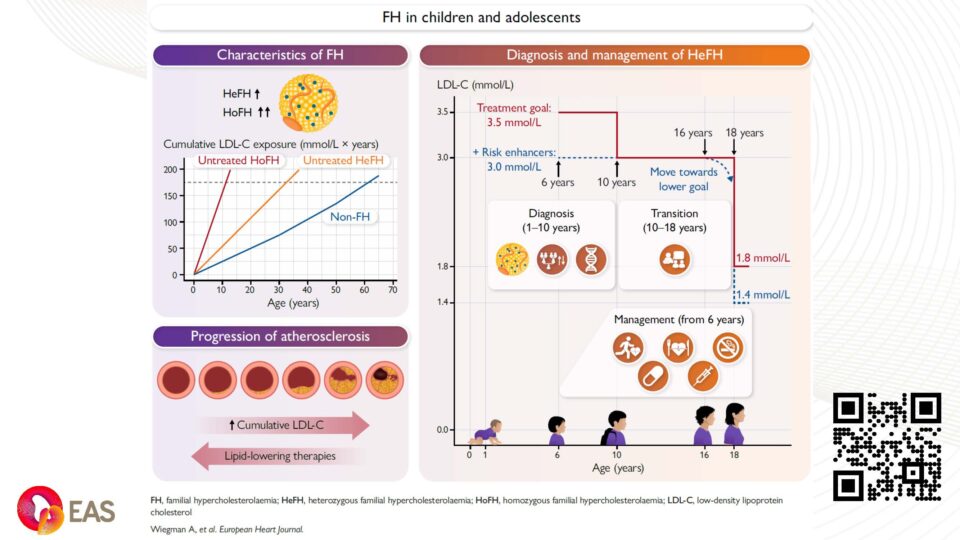
The new consensus statement highlights the need to improve the detection and management of familial hypercholesterolaemia (FH) in children and adolescents. The panel proposes widespread paediatric screening, earlier treatment, and updated approaches to diagnosis and care.
FH is a common genetic disorder characterised by lifelong elevated low-density lipoprotein cholesterol (LDL-C), which increases the risk of premature atherosclerotic cardiovascular disease (ASCVD). FH occurs in two forms: Heterozygous FH (HeFH), affecting approximately 1 in 300 people worldwide, and the rarer Homozygous FH (HoFH), affecting around 1 in 300,000. Individuals with HoFH, if untreated, are at extremely high risk of cardiovascular complications, already in childhood.
In the decade since the 2015 EAS consensus statement on FH in children, knowledge of the pathogenesis of FH has increased markedly, and a wider range of LLTs is now available (although access and reimbursement remain country-specific). This updated EAS consensus statement, co-chaired by professors Albert Wiegman and Jeanine Roeters van Lennep, provides revised diagnostic criteria, updated LDL-C treatment goals, and practical guidance on managing FH in children and adolescents. It emphasises the importance of starting LLTs early, ideally from the age of 6 for children with the HeFH and from the time of diagnosis for the children with the HoFH, and provides treatment algorithms for both HeFH and HoFH. The statement also addresses the transition to adult care and implementation strategies.
What is new in this EAS consensus statement?
- Updated diagnostic criteria to improve diagnostic sensitivity
- Proposed lower age to start treatment
- Proposed lower LDL-C treatment goals, made possible by the availability of new LLTs
- Emphasis on the importance of reducing cumulative LDL-C exposure
- Updated treatment algorithms and the latest evidence supporting the use of novel LLTs
- Proposals to facilitate improved transition to adult care and implementation strategies?
Over the past decade, major advances in understanding FH have been accompanied by the development of a broader range of LLTs. Despite this progress, FH remains underdiagnosed and undertreated, particularly in children where it is rarely identified despite being one of the most common inherited conditions. “This is a missed opportunity, because we now have highly effective treatments that can normalise cholesterol levels and prevent cholesterol from accumulating in the arteries when started early in life.” says Co-Chair of the consensus and Trustee of FH Europe Foundation, Prof. Albert Wiegman (Netherlands).
Broader cardiovascular health implications
This important consensus statement comes at a very timely moment, following the announcement of the EU Safe Hearts Plan, where significant emphasis is being placed on cardiovascular health (CVH), early prevention, child health, and screening. With the recent call for evidence for cardiovascular health checks, the publication marks another important and highly practical set of evidence-based clinical recommendations for tackling cardiovascular disease (CVD) from early in life.
To address gaps in diagnosis, the EAS consensus panel proposes updated diagnostic criteria aimed at improving detection rates in younger populations. The panel also encourages all countries to establish paediatric screening programmes for FH.
Systematic screening approaches, including family cascade screening and universal paediatric screening in the first decade of life, have been shown to improve detection rates and to be cost-effective, but are not consistently used worldwide. “We cannot rely on chance diagnosis in adulthood,” says Co-Chair of the consensus and Scientific Advisor of FH Europe Foundation, Prof. Jeanine Roeters van Lennep (Netherlands). “Systematic screening is essential to find children with FH early and intervene effectively.”
Furthermore, the paper recommends testing for lipoprotein(a) [Lp(a)] in all children with suspected FH at the same time as paediatric screening, but not before 5 years of age.
We are delighted to share that Magdalena Daccord, FH Europe Foundation’s CEO, was one of the reviewers of the consensus statement.
Read:
2.Lipid clinics worldwide: harmonization and guidance on how to optimally organize and fund: a European Atherosclerosis Society consensus statement across 55 countries and more than 500 lipid clinics
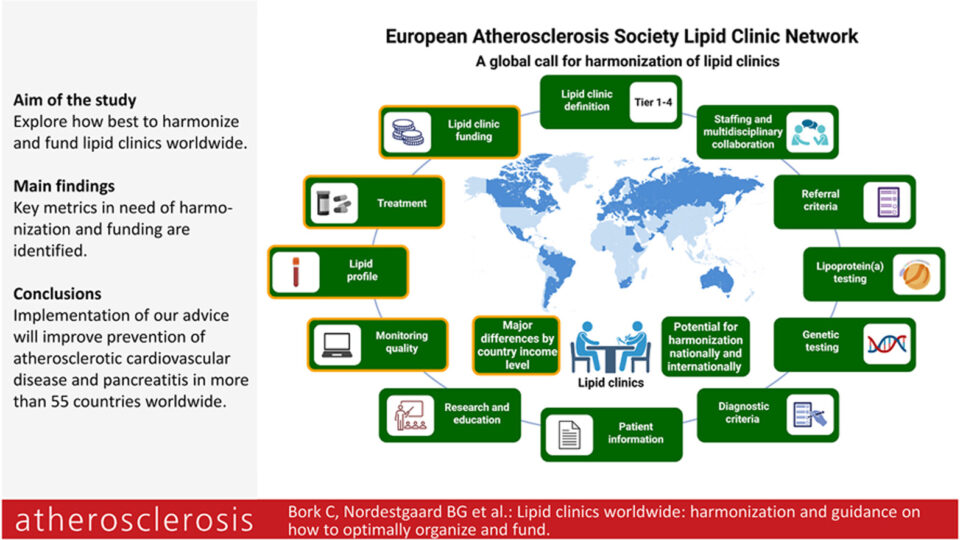
Atherosclerotic cardiovascular disease (ASCVD) remains the leading cause of death worldwide, responsible for one in three deaths globally. Despite major advances in lipid testing, preventive therapies, and international treatment guidelines, implementation of optimal lipid management remains highly uneven across countries and healthcare systems.
Lipid clinics offer specialist care to patients at highest ASCVD risk and with rare lipid disorders. They play a key role in increasing and improving education about lipid disorders among other healthcare professionals, in organisation of national registries, and in promoting awareness of the societal benefits and reduced costs of improving prevention of ASCVD. The EAS-Lipid Clinic Network has been established so that lipid clinics from all over the world can work together to tackle shared challenges and learn from mutual exchange.
This new consensus statement from the EAS Lipid Clinic Network, involving more than 500 lipid clinics in 55 countries, highlights one of the LCN's main aims - the need to harmonise the diagnosis and management of lipid disorders globally.
Co-chair of the statement, Dr Christian Bork (Denmark) said: ‘We identified major differences between clinics, nationally and internationally, in the delivery of guideline-recommended patient care. While almost all clinics followed guidelines, there were issues with implementation, especially for diagnostic testing, treatment and follow-up. We have excellent evidence-based guidelines on dyslipidaemia, and developing more guidelines is not the answer. Instead, we need to focus on how we organise and operate lipid clinic networks to ensure harmonised patient care, adapting to the realities of access and funding across different regions.’ Co-chair and EAS President, Prof. Borge G. Nordestgaard (Denmark) added: ‘Harmonisation is crucial to ensure optimal patient care, and ultimately to reduce the burden of preventable cardiovascular events such as heart attacks and strokes.’
Based on the 2024 EAS Lipid Clinic Network survey, the paper identifies several key areas for improvement, including increased education nationally and internationally, harmonisation of clinic organisation and treatment, guidance on staffing, development of national registries, and structured dialogue with governments to support funding and reduce the healthcare burden of ASCVD.
The consensus marks an important milestone for the clinical and patient communities by prominently including lived experience and a patient perspective. Elsie Evans, FH Europe Foundation Ambassador Programme Manager and a person living with HoFH, has been involved right from the beginning as an author of the publication.
The consensus statement provides practical recommendations for establishing well-functioning lipid clinic networks, including standards for diagnosis, treatment, multidisciplinary collaboration, education, and funding, with a particular focus on improving care in regions with high cardiovascular burden.
Read:
Together, these two EAS consensus statements reinforce the urgent need for a life-course, systems-based approach to cardiovascular prevention, from early screening and detection in childhood to equitable access to specialised lipid care across healthcare systems. They represent an important step towards reducing the burden of preventable cardiovascular disease worldwide.