We are delighted to welcome to our team Reante Kaal-Poppelaars, as our Project Manager for Internal Processes. We could not be more excited, as with the growth of the organisation we want to put in place robust processes to be more effective and efficient. Another reason to celebrate is the fact that Renate is joining the FH Europe Foundation as our first volunteer in the project team, demonstrating our commitment to building opportunities for volunteers within our operational structures.
Renate will lead activities focusing on internal processes review and improvements, organising FH Europe Foundation’s SharePoint, and laying the groundwork for a customer relations management tool (CRM) implementation. With a passion for making a difference in the lives of those affected by inherited lipid disorders and having a personal family experience with it, she is eager to apply her professional experience, skills and knowledge to help streamline the Foundation's operations and enhance the team's impact.
"I am deeply motivated to join the FH Europe Foundation, not only to share my experiences but also to learn from this community. Having lived through the challenges and revelations of managing elevated Lp(a) within my own family, I understand the importance of support, awareness, and education in navigating these health issues. This year I turned 54 and the stark reminder is that my father passed away from a heart attack at the age of 53—a milestone I have now passed. I look forward to collaborating with the Foundation, its members, and the wider community to contribute to our collective efforts in improving patient care and outcomes. Together, I believe we can make a significant impact." says Renate about her motivation to join the FH Europe Foundation.
About Renate
Her connection to the cause of FH Europe is very personal. Living in the Netherlands with her husband, Edwin, and their children, Aedan and Indy, her family has navigated the complexities of FH and elevated Lp(a). While she was relieved to discover that their children did not inherit Edwin's FH, she learned that Aedan and herself both have elevated Lp(a), a revelation that has explained much of their family's medical history, including her father's heart health challenges. This journey has brought their family closer and intensified her commitment to health awareness and support for those on similar paths.
In addition to her role at FH Europe, Renate is involved in running her family's company. Her career path before joining the family venture had been varied, spanning several key industries. She had held positions as a Project Manager and in managerial roles within banking, healthcare insurance, and medical services in Amsterdam, as well as with the Amsterdam municipality. A consistent theme in her career has been her gravitation towards creating and enhancing organisational structure. In her spare time, she loves reading, spending time with her family, and walking her three dogs.
"I could not be more thrilled to be able to bring to our team someone like Renate. Her joining as a volunteer demonstrates the value we create to the community in a greater sense. Since coming on board, Renate brought a lot of enthusiasm and excitement to our team about getting our processes sorted. That is a good sign and a very critical step in our growing organisation!" – added Magdalena Daccord, FH Europe Foundation's CEO.
Brussels 14 March 2024: The European Alliance for Cardiovascular Health (EACH) welcomes the recent announcement by the European People’s Party to include a ‘European Cardiovascular Health Plan’ as a core component of their electoral manifesto.
“We are launching a European Cardiovascular Health Plan because we know that cardiovascular disease is the biggest killer in the EU. This plan should include a European Knowledge Centre and promote a joint cardiovascular and diabetes health check.” European People’s Party (EPP) Manifesto full version can be found here.
This historic step answers the urgent need for comprehensive action to address Europe’s health crisis and tackle its leading cause of death – cardiovascular disease which costs the EU €282 billion every year. The long-term mission to achieve a healthier Europe was the reason why the European Alliance for Cardiovascular Health (EACH) was created in 2021 as a coalition of patients, healthcare professionals, researchers, and health industry representatives.
The inclusion of cardiovascular health in the EU electoral manifesto comes after two years of effort by EACH partners to advocate for a comprehensive EU policy response. In December 2023, the EACH exhibition Vote Cardiovascular Health 2024 took place in the European Parliament. The exhibition showcased the burden of cardiovascular diseases in figures per each EU Member States. The very urgent public topic, advocacy efforts on the national level as well as the engaging and innovative format of the event attracted over 100 Members of the European Parliament (MEPs) from 20 countries, who pledged action at both the EU and national level.

Emma Print (FH Europe Foundation) conducting a video interview with Ulrich Janßen, a patient representative from Germany.
MEP Łukacijewska, Co-host of the event, signing the Pledge wall.

Marc Rijken together with his wife Manon and daughter India, delivered a powerful and a very emotive closing speech along with three other fellow patients at the Opening Ceremony.

The EACH Cardiovascular Health Plan for Europe was launched in May 2022. Its key goals are to:
To achieve this, the focus will need to be on primary prevention at the population level, improvements in secondary prevention through timely detection, equal access to high-quality patient-centred healthcare, and increased uptake of rehabilitation.
More specifically, EPP calls for the European Knowledge Centre and European Cardiovascular Health Check as an integral part of the EACH proposed Vision.
A European Cardiovascular Health Data Knowledge initiative aligns with the European Health Data Space to establish a unified system for cardiovascular data. By integrating various sources of information, including registries and patient-generated data, this effort aims to enhance connectivity, promote collaboration across borders, and facilitate research and innovation in cardiovascular health. Similarly implementing European Cardiovascular Health Checks for common risk factors (including among several biomarkers LDL cholesterol and elevated Lp(a)), and with due consideration to gender differences, can help diagnose early, prevent disease, promote cardiovascular health (CVH), and save healthcare costs.
EACH believes that a dedicated Cardiovascular Health Plan that covers the full spectrum of cardiovascular health during a person’s entire life, can alleviate the burden of CVD on millions of people. It will also benefit societies and economies and will have a trickle-down effect engaging the whole cardiovascular health community with the creation of national CVH plans that are tailored to national contexts and needs.
“In addition to awakening the political will to tackle this serious health challenge, we need a paradigm shift in how the stakeholders are currently engaging. All stakeholders need to engage (...) to tackle cardiovascular health (...) in ways they have never done before.” EACH Patient Representative.
Read the official EACH press release.
As we mark World Obesity Day, it's important to recognise that obesity isn't just a matter of appearance or lifestyle—it's a significant risk factor for heart disease, even among those whose heart disease risk is mainly driven by genetically high cholesterol.
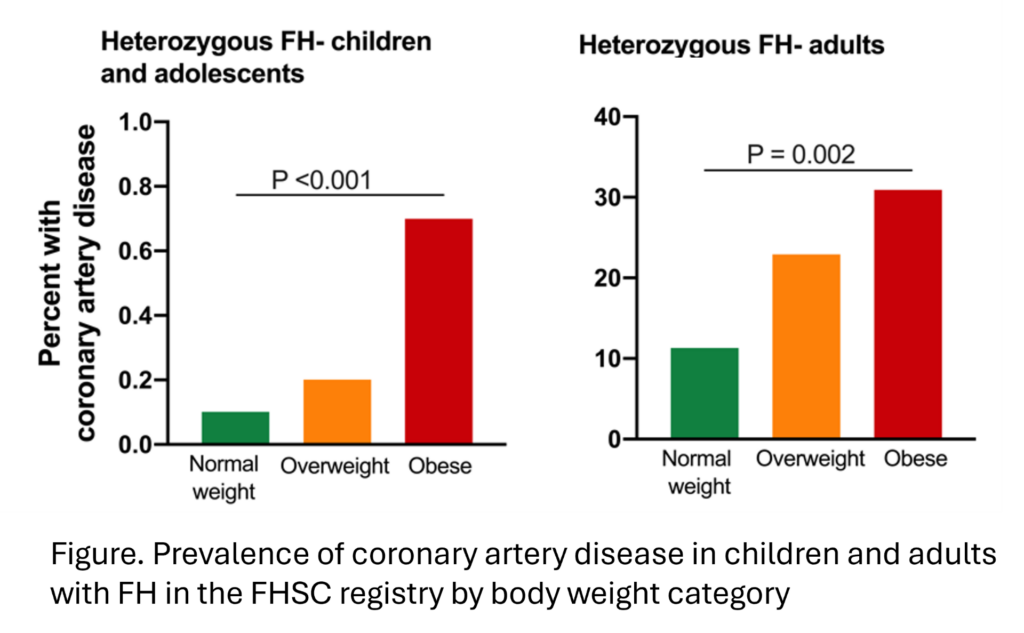
Approximately one in three hundred (1:300) people has familial hypercholesterolaemia (FH), the most common monogenic disorder. In these individuals, a genetic defect in cholesterol uptake leads to lifelong elevation of low-density lipoprotein (LDL)cholesterol, and, hence, an increased risk of heart disease. A study conducted by Dr Amany Elshorbagy, on behalf of the FH Studies Collaboration (FHSC) Investigators, sheds light on the relationship between obesity and atherosclerotic cardiovascular disease (ASCVD) in individuals with heterozygous FH (HeFH). This study, published as a congress abstract in the Atherosclerosis Journal, involved over 35,000 patients with HeFH across 50 countries from 6 continents.
The researchers aimed to determine the prevalence of overweight and obesity among these individuals and whether they pose additional risks for ASCVD beyond their high cholesterol levels.
They found that, globally, more than half of adults and over a quarter of children with HeFH were either overweight or obese. The prevalence was particularly high in Northern Africa and Western Asia, highlighting a health concern.
Importantly, the study found that obesity was associated with a more atherogenic lipid profile, indicating a higher likelihood of plaque buildup in the arteries, even when individuals were on lipid-lowering medication. Obesity was linked to a significantly higher likelihood of coronary artery disease and stroke in adults, and coronary artery disease in children. These associations remained even after controlling for other risk factors such as diabetes, hypertension, and smoking.
This suggests that obesity exacerbates the already augmented risk of heart disease in people with HeFH.
The findings from this study are briefly explained in a podcast by Medical Digest, and a press article by Medscape, with commentary from other experts in the field.
It underscores the critical importance of weight management, even in individuals whose cardiovascular risk is primarily driven by genetic cholesterol elevation. While medications can help control cholesterol, addressing obesity is also vital in reducing the risk of heart disease in this population.
Sustained efforts to maintain a healthy weight through a balanced diet, regular exercise, and lifestyle modifications are imperative for all. By prioritising weight management, we can mitigate the risk of heart disease not only in the general population but also in those with genetically high cholesterol levels.
Prepared by Dr Amany Elshorbagy

To learn more about obesity, and the links between obesity, childhood obesity and genetically high cholesterols check out the resources below.
This research by EAS FHSC and Dr Amany Elshorbagy adds to the existing body of evidence which suggests that early screening and detection are key to preventing lasting health implications. It also ties in very strongly with our ongoing efforts to engage political support and to build synergies to successfully tackle CVD risk factors, as early as possible, starting in childhood.
On the occasion of the World Obesity Day, we also wish to bring to your attention the Zagreb Declaration.
The Zagreb Declaration, adopted on 10 May 2023, sets out a political roadmap for reversing the rapid rise of childhood obesity. It acknowledged the importance of raising awareness about obesity and how this issue affects children and future generations and recognized the necessity of leadership and advocacy to accelerate actions to stop childhood obesity at national and international levels on all concerned platforms and relevant international fora.
Back in 2022, we published the Prague Declaration on FH paediatric screening and preventing the preventable.
For more information on obesity and the world awareness campaign, check out https://www.worldobesityday.org/.
Learn more about the updates from EAS FHSC and the EAS 2023 congress by watching our webinar, where Dr Amany Elshorbagy explained her research https://www.youtube.com/watch?v=PAwXf6cO6sk.
Reference:
Elshorbagy A, et al. Global prevalence of overweight and obesity among paediatric and adult patients with homozygous or heterozygous familial hypercholesterolaemia, and association with coronary artery disease. Atherosclerosis 2023; 379 Supplement: S15. DOI: https://doi.org/10.1016/j.atherosclerosis.2023.06.925.