FH Awareness Day 2023 is about engaging and empowering the wider community in the mission for cardiovascular health (CVH).
Cardiovascular disease (CVD) is a general term for conditions affecting the heart or blood vessels. They include coronary heart disease, cerebrovascular disease, peripheral arterial disease, rheumatic heart disease, congenital heart and deep vein thrombosis and pulmonary embolism[1].
CVDs are the leading cause of death globally, with over three quarters of them taking place in low- and middle-income countries. In 2019, they caused 18.6 million deaths worldwide . It represented over 32% of all global deaths, where 85% of them were due to heart attack and stroke.
The burden of disease continues. In 2019, nearly 400 million years of healthy life (quantified as disability-adjusted life years or DALYs) were lost due to cardiovascular disease (CVD). This marks a 24% increase in the global CVD burden compared to 2000 (316.9 million DALYs)[2].
And yet, up to 80% of CVDs can be prevented[3] , provided the underlining causes can be identified and effectively addressed. In some cases, this means addressing behavioural risk factors such as tobacco use, unhealthy diet and obesity, physical inactivity and harmful use of alcohol. In other cases – like the CVD caused by familial hyperlipidemias, the key lies in early screening, detection and appropriate management (incl. lifestyle modifications and therapies). However, to achieve meaningful results the engagement and collaboration between the wider community of multidisciplinary stakeholders is critical.
FH stands for Familial Hypercholesterolaemia and means genetically caused very high LDL cholesterol. It is the world’s most common, monogenic condition. This serious CVD risk factor affects over 30 million people worldwide, and 2.5 million people in Europe, of which 500’000 are children. Undetected and unmanaged FH can lead to atherosclerosis and early cardiovascular disease including premature heart attacks and even death. Despite being named by the WHO a Global Public Health Burden over a quarter of a century ago, it is still very poorly diagnosed and ineffectively managed. Based on the available data from the global FH registry, it is estimated that only 10% of the affected people have been identified to date. In other words, 9 out of 10 people with FH do not know they have it and are not appropriately managing their very serious CVD risk factor.
Once FH is appropriately diagnosed and managed, those living with the condition can live a long and "normal" life. Those diagnosed early in childhood adopt easily the new lifestyle, where taking daily medication and adhering to simple rules – no smoking, physical activity and a healthy low-fat diet - are just a part of daily life.

Every year, on September 24th, FH Awareness Day is observed. It takes place 5 days before World Heart Day.
This year, the FH Europe Foundation together with the Network of patient organisations, patient ambassadors, medical experts, supporters, and friends is engaging the international community to raise awareness, educate and to advocate for a change which has the potential for a tremendous shift – from cardiovascular disease to cardiovascular health.
FH Europe Foundation is embarking on a three-pronged approach to drive awareness for FH Awareness Day. Providing three very different yet complementary elements allows us to reach a wider audience.
The theme running throughout the whole FH Awareness campaign is meant to put the people with FH at the heart of all activities. “People Like Us” is about stories told by patients, and images of real patients. Over the course of one month they will be educating, advocating, sharing. Starting with the social media campaign People Like Us, explains that FH is an invisible disease, and it doesn’t matter who you are, what you look like, your age, gender, or ethnicity. You can be affected if you inherited it. A toolkit with basic social media assets, building on simple messages, scientifically validated, and using images of everyday situations and people including the patients from the FHEF network aims at addressing wider, international public. The campaign has been translated into 13 languages and is being shared from August 24th on social media in collaboration with the Network members across Europe, and organisations in South America, Middle East and Australia.

This year, for the first time, FH Europe Foundation is collaborating very closely with the European Atherosclerosis Society (EAS) on an unconventional educational programme aimed at the international members of EAS community. For the duration of a week, a series of 5 webinars of 30min, will be hosted live with patient ambassadors and advocates partnering with researchers and clinicians as speakers and moderators. From topics of Genetics, Combined testing for other CVD risk factors (elevated Lp(a)), Access to novel treatments, to more unusual ones like focusing more on social sciences and policy like Screening and the EU CVH policy, Challenges faced by children with FH – the medical community will be exposed to new learnings …through the lens of the patients and citizens.

On 21st September, FH Europe Foundation will be hosting a webinar with 7 international female panelists (why not?). The discussion, rather than a series of slide presentations, will be moderated by a Patient Ambassador, living with FH and elevated Lp(a). Among the 6 female speakers is the leading researcher and advocate for greater research about women and CVD/FH/pregnancy. She is a young generation champion researcher and clinician from Germany, combining her experience to inform better health policies. We have 4 female patients and fierce advocates who between them have a number of misdiagnosed heart attacks, experienced gaslighting in the interactions with clinicians and the community. Make sure you join them by registering now. The topic of the webinar "FH and the gender bias - misdiagnosed and under treated".
Many biases exist in the healthcare system including the mistaken belief that women are more protected from heart disease due to oestrogen levels. In addition, FH is commonly misunderstood, and standard risk calculators do not take into consideration the increased risk of FH due to lifelong high cholesterol. The onset of atherosclerotic cardiovascular disease (ASCVD) occurs 20 years earlier in women with FH than in those without FH.[4][5]
The combination of the social media campaign and the webinar is meant to help relaunch a dedicated ‘Women and FH Survey’, as the existing research and data gap on how FH affects women, their family planning decisions as well as health pre-, during and post pregnancy is enormous. The survey is available in 16 languages, and the goal is to collect 1000 responses.
This September, it will be one year since the publication of the of Prague Declaration on Achieving FH Paediatric screening across Europe[6]. The high-level policy document, launched under the Czech EU Presidency as a result of a Senate meeting in Prague in 2022, was endorsed by the Czech Ministry of Health. It built on recognition of the European Commission of FH Paediatric Screening as a Public Health Best Practice and the high-level technical meeting from 2021, under the Slovenian EU Presidency, which led to 2 scientific publications.
The Prague Declaration has been presented across Europe, in various scientific and policy and advocacy meetings. It even made its way to the National Lipids Association meeting in the USA. To date is has been endorsed by over 100 individuals including EU politicians, scientists, medical experts, patient organisation leaders and individual patients plus over 60 organisations from the World Heart Federation, the European Alliance to Cardiovascular Health, the European Public Health Alliance and European Connected Health Alliance to international medical societies, national patient organisations and medical universities[7]. It serves as a blueprint for FH screening programs and national CVH Plans in Czechia, Austria, Bulgaria, Cyprus, Poland, Germany, France, Spain.
The impact of the Prague Declaration and related advocacy and policy influencing in the space of FH early detection and CVD prevention has been recognised and appreciated internationally, offering bigger opportunities and possibilities, leading to a paradigm shift from Cardiovascular Disease towards a global concept of Cardiovascular Health (CVH).

And so, the FH Awareness Day efforts will conclude at the United Nations General Assembly (UNGA) Science Summit[8] in New York, on September 26th, where the FH Europe Foundation team will be addressing an international multidisciplinary community, talking about innovation, health data and digitalisation in the context of improved FH screening, CVD prevention implementation in very specific terms, referred to in the document, and unquestionably contributing to the CVH promotion on the international and national level. (You can register here to join online or in person).
FH Europe Foundation proud to support Apheresis Awareness Day 2023!
We want to raise awareness about the benefits of apheresis therapy in managing conditions like homozygous familial hypercholesterolemia (HoFH) and high Lp(a) as well as the rare condition familial chylomicronemia syndrome (FCS). We want to highlight the crucial role of apheresis in reducing the risk of cardiovascular events in patients with inherited lipid conditions as well as reducing the risk of acute pancreatitis during pregnancy in patients with FCS. This campaign will grow and we encourage you to share some of your stories. [1]
Learn more about Apheresis and watch the stories from our patients, who are involved in this treatment.
Apheresis treatments for inherited lipid conditions are therapeutic procedures that aim to lower the levels of lipids, such as cholesterol or triglycerides, in the blood. During the procedure, blood is collected from a patient and passed through a machine that separates the plasma from other blood components. In HoFH and Lp(a) the machine then removes the excess lipids from the plasma and returns the remaining blood components to the patient, while in FCS the patient has given donated plasma. This process can be done on a weekly or bi-weekly basis, and each treatment session typically lasts a few hours.

Proteins carry cholesterol throughout the body, forming a combination called lipoprotein. There are two main types of lipoproteins: LDL (low-density lipoprotein), which is harmful and previously referred to as “bad’ cholesterol, and HDL (high-density lipoprotein), which is protective and previously referred to as "good" cholesterol. If you have too much harmful cholesterol in your blood, your risk of getting cardiovascular (heart) disease increases. Another lipoprotein, Lp(a), can also increase the risk of cardiovascular disease if it is raised.
Lipoprotein apheresis is a highly effective procedure designed to remove LDL cholesterol from the bloodstream. This intervention is known to cause only a minimal decrease in HDL levels. It is recommended for individuals who have very high LDL cholesterol levels and already attempted medication therapy and a low-cholesterol diet, but levels of LDL cholesterol remain high.
Moreover, it is the preferred approach for managing elevated Lp(a) levels.
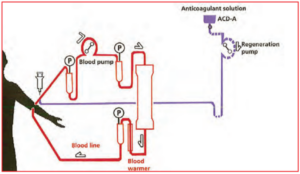
The diagram shows how lipoprotein apheresis is performed.
Apheresis treatments have been shown to effectively reduce lipid levels in patients with inherited lipid disorders, helping to prevent complications such as cardiovascular disease. It is also a treatment used to support patients living with the rare condition FCS during pregnancy.
Lipoprotein apheresis could be an option for you, if:
Lipoprotein apheresis treatment can be done on a weekly or bi-weekly basis, and each treatment session typically lasts a few hours. Patients are treated on an individual basis at a specialized treatment facility. This will also impact on how regular treatments can happen.
Plasma exchange for patients with familial chylomicronemia syndrome (FCS) during pregnancy involves the removal of plasma components that contribute to high levels of triglycerides. By removing excessive triglycerides, this treatment helps reduce the risk of pancreatitis and other complications associated with FCS during pregnancy. The frequency and duration of these treatments vary depending on the patient's condition and response to therapy. Typically, patients undergo treatment once or twice a week for a few hours each session. These treatments can greatly improve the health and well-being of FCS patients during pregnancy. [2]

Apheresis offers hope to patients with high Lp(a) levels and signs of atherosclerosis. [3]
Listen to Krish, an FCS patient from the UK, talking about her experience having lipoprotein apheresis during her pregnancy.
Lipoprotein apheresis can be used for treating children. It means it’s possible to stop high cholesterol from causing damage at an early age. This is important for people with FH with two faulty genes (Homozygous FH, Compound HeFH), which can cause heart disease early in life if it isn’t treated.[4]

Patient Ambassador Avery (age 15) started with apheresis treatments at age 7.
Access to this specialized treatment is very different, depending on the location. It varies not only among countries but also inside every country.
In many areas, the availability of Lipoprotein Apheresis is very limited, largely attributable to the procedure's high cost and the specialized apparatus required. In addition, there is a lack of trained medical professionals who are able to perform this complex procedure, further restricting access for those in need. This also places a higher burden on patients both socially, financially and emotionally.
Inaccessibility to lipoprotein apheresis for example has dire consequences for patients in Lebanon with conditions like Homozygous FH, Lp(a), and FCS during pregnancy. [5]
Listen to Chyrel, our Patient Ambassador living with HoFH talking about problems with limited access to Apheresis treatment in Lebanon.
Lipoprotein apheresis is a procedure that's similar to kidney dialysis. During the procedure, two needles (called cannulae) are inserted into your veins. One needle is used to lead the blood flow from the body and the other is used to return the treated blood back into your body. A portion of your blood is circulating outside of your body using a machine. This machine removes LDL cholesterol and Lp(a) from your blood, and then returns the treated blood back into your body. The machine parts that come in contact with your blood are sterile and are only used once.

In the beginning, your LDL cholesterol and/or your Lp(a) levels will be measured before and after each apheresis treatment. Your blood results will also regularly be reviewed and your treatment will be adjusted as needed to ensure it's working as optimal as possible.
With just one session, lipoprotein apheresis can lower your LDL cholesterol and Lp(a) levels by 50 and up to 70 percent, depending on your initial levels and the amount of blood treated. However, it doesn't address the root cause of high LDL cholesterol and/or high Lp(a). Your levels will start to rise again soon after treatment. To maintain lower levels of LDL/Lp(a), you'll need treatment every two weeks or, in some cases, weekly. Lipoprotein apheresis seems to be a lifelong therapy, so it's important to continue following a low-fat diet and taking all cholesterol medications.
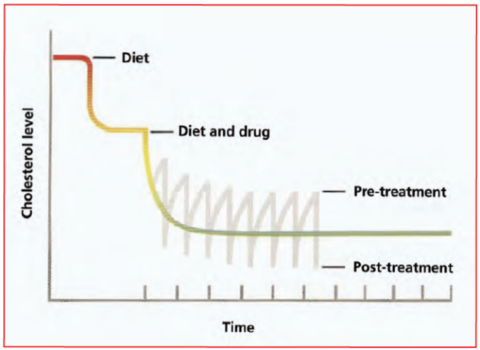
The diagram - combination of diet, medication, apheresis treatment lower cholesterol.
If you have issues with blood flow from your arm veins, you may be offered:
If you need either of these, your doctor will discuss both options with you in more detail.
Heparin or another anticoagulant solution, called ACD-A, can be used to thin your blood before it circulates through the machine.
The blood-thinning medication prescribed will be determined by the type of machine that is used. A temporary decrease in your blood calcium levels may be caused by ACD-A. To prevent this, calcium tablets will be provided to you during each treatment session.
A small number of patients may experience one or more of the following temporary side effects:
The nurses in the unit will be able to help treat any problems or side effects.
For patients with HoFH and Lp(a) you will be advised not to take any beta blocking tablets, including atenolol, propanolol, metoprolol, and bisoprolol, or any other medication to lower your blood pressure before your treatment. You should continue taking your medication as usual the day after your treatment. If you develop anaemia, you may need to take an iron supplement.
If your doctor suggests starting ACE inhibitor medication, such as ramipril, lisinopril, and perindopril, please discuss the effects with him or consult your lipid specialist, as they may interfere with some of the machines used for lipoprotein apheresis. If you are already taking ACE inhibitor medication before starting apheresis, your doctor may need to switch you to an alternative medicine that does not interfere with the machine before starting treatment.
It is important to eat and drink something before your treatment, and you may continue to eat and drink during the procedure. However, please avoid alcohol 24 hours before your treatment, as well as any strenuous exercise on the day of your treatment, and activities that may increase the risk of physical injury for 24 hours after your treatment due to the blood-thinning medication used.
For the first two or three occasions, we recommend that you do not drive to and from your treatment. To further reduce the risk of side effects, it is advisable to rest for the remainder of the day after your treatment.